Phosphate homeostasis, monitoring and managment of hyperphosphatemia in patients with the Chronic Kidney diseases
1. Phosphate homeostasis
Phosphate is an abundant mineral found in the body. The body store of phosphate is 500 to 800 g, with 85% of the total body phosphate present in crystals of hydroxyapatite in the bone — about 10% found in muscles and bones in association with proteins, carbohydrates, and lipids. The rest gets distributed in various compounds in the extracellular fluid (ECF) and intracellular fluid (ICF). Phosphate is predominantly an intracellular anion.
The normal plasma inorganic phosphate (Pi ) concentration in an adult is 2.5 to 4.5 mg/dl, and men have a slightly higher concentration than women. In children, the normal range is 4 to 7 mg/dl. A plasma phosphate level higher than 4.5 mg/dL is hyperphosphatemia.
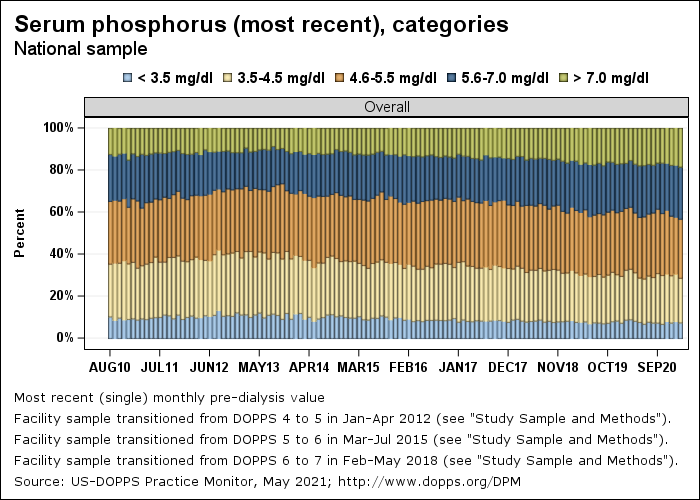
It is possible to achieve normal levels of phosphorus in the blood of patients on dialysis only in 40-50%.
Figure. Serum phosphorus of patients on dialysis (USA)
Phosphate plays an essential role in many biological functions such as the formation of ATP, cyclic AMP, phosphorylation of proteins, etc. Phosphate is also present in nucleic acids and acts as an important intracellular buffer.
Normal adult dietary phosphate intake is around 1000 mg/day. 90% of this is absorbed primarily in the jejunum. In the small intestine, phosphate is absorbed both actively and by passive paracellular diffusion. Active absorption is through sodium-dependent phosphate co-transporter type IIb (NPT2b).
Figure. Transepithelial phosphate transport in the small intestine.
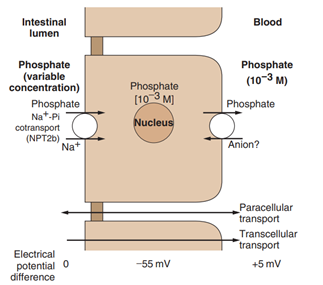
(Phosphate enters the enterocyte (influx) through the brush border
membrane using the Na+
/Pi cotransport system, with a stoichiometry
of 2 : 1, operating against an electrochemical gradient. Phosphate exit
at the basolateral side possibly occurs by passive diffusion or more
probably by anion exchange)
Kidneys excrete ninety percent of the daily phosphate load while the gastrointestinal tract excretes the remainder (Figure).
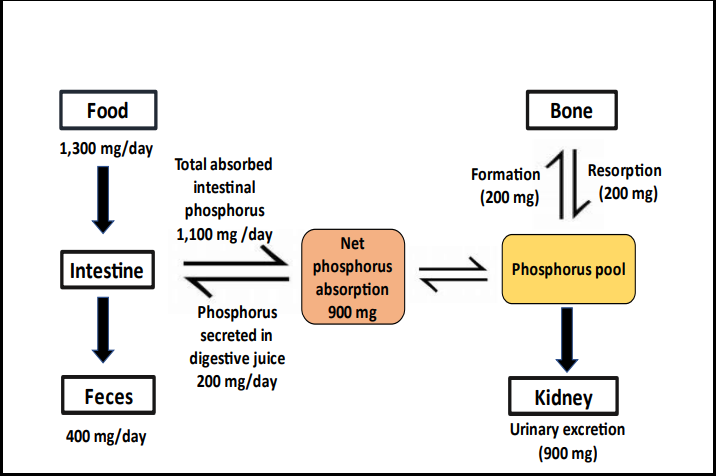
Figure - Phosphorus homeostasis in healthy adults (Dr. David St-Jules., 2022)
As phosphorus is not significantly bound to albumin, most of it
gets filtered at the glomerulus. Therefore, the number of functional nephrons
plays a significant role in phosphorus homeostasis; 75% of filtered phosphorus
is reabsorbed in the proximal tubule, approximately 10% in the distal tubule,
and 15% is lost in the urine. In the luminal side of the proximal tubule, the
primary phosphorus transporter is the Type II Na/Pi co-transporter (NPT-2a).
The activity of this transporter is increased by low serum phosphorus and
1,25(OH)2 vitamin D, increasing reabsorption of phosphorus. Renal tubular
phosphorus reabsorption also increases by volume depletion, chronic
hypocalcemia, metabolic alkalosis, insulin, estrogen, thyroid hormone, and
growth hormone. Tubular reabsorption of phosphorus decreases by
parathyroid hormone, phosphatonins, acidosis, hyperphosphatemia, chronic
hypercalcemia, and volume expansion.
Phosphorus is transported out of the renal cell by a phosphate-anion exchanger located in the basolateral membrane.
Phosphate homeostasis is under direct hormonal influence of calcitriol, PTH, and phosphatonins, including fibroblast growth factor 23 (FGF-23). Receptors for vitamin D, FGF-23, PTH, and calcium-sensing receptor (CaSR) also play an important role in phosphate homeostasis. Serum phosphate level is maintained through a complex interaction between intestinal phosphate absorption, renal phosphate handling, and the transcellular movement of phosphate that occurs between intracellular fluid and bone storage pool. A transient shift of phosphate into the cells is also stimulated by insulin and respiratory alkalosis.
Dr. David St-Jules. A Systematic Review of Online Resources on Dietary Management of Hyperphosphatemia in People with Chronic Kidney Disease (CKD). University of Nevada, Reno. December,2022